6204 - Peripheral vestibular disorders
DBQ: Link to Index of DBQ/Exams by Disability for DC 6204
Definition
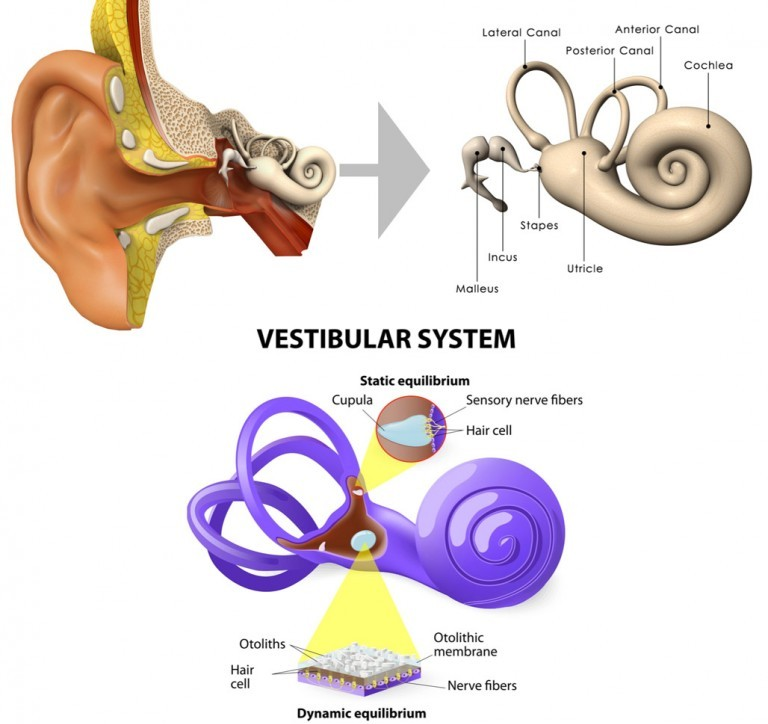
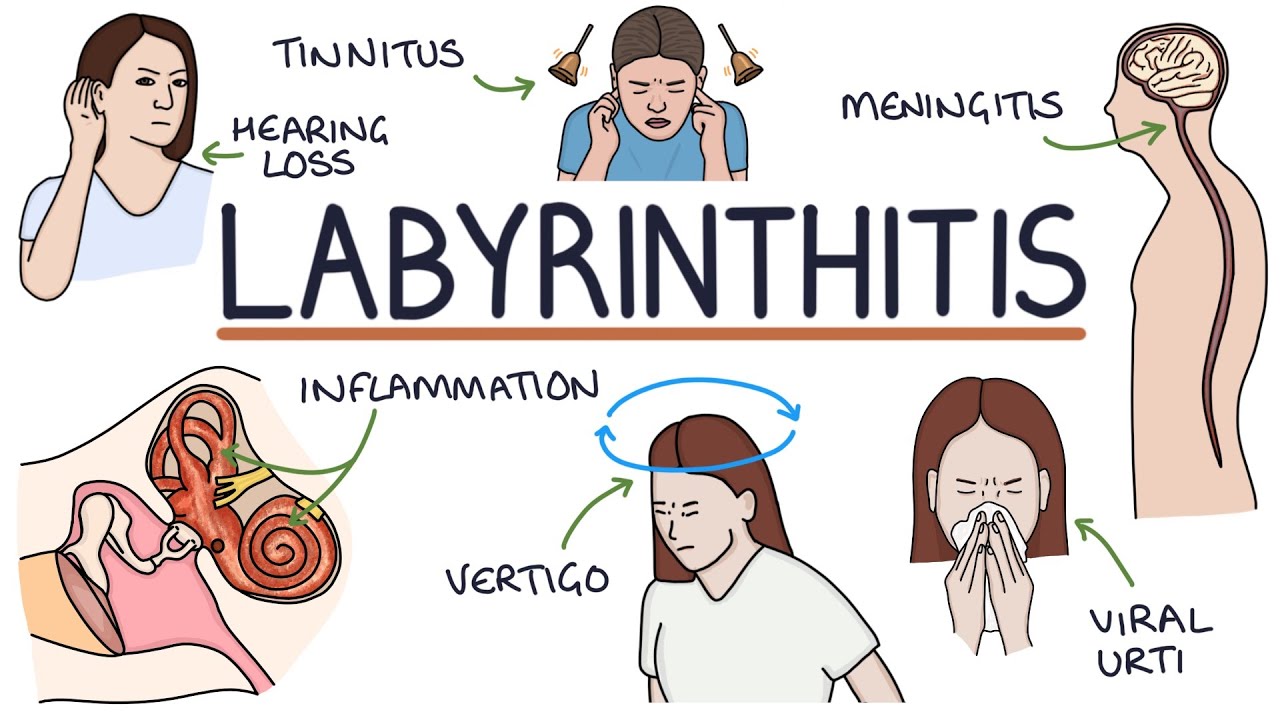
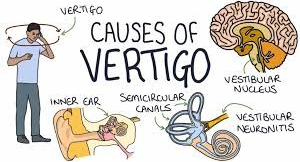
The vestibular apparatus is responsible for maintaining equilibrium. The labyrinth is part of this system. There are two common conditions that may occur as result of abnormal functioning of the vestibular apparatus or the labyrinth: vertigo and labyrinthitis. Vertigo is the sensation of spinning movement in relationship to the environment associated with imbalance and difficulty walking. Vertigo may also be referred to as dizziness, lightheadedness, or giddiness. Labyrinthitis is inflammation of the labyrinth, a series of intricate communicating passages of the inner ear that contain the receptors for equilibrium.
{kind=link}
{kind=link}
Etiology
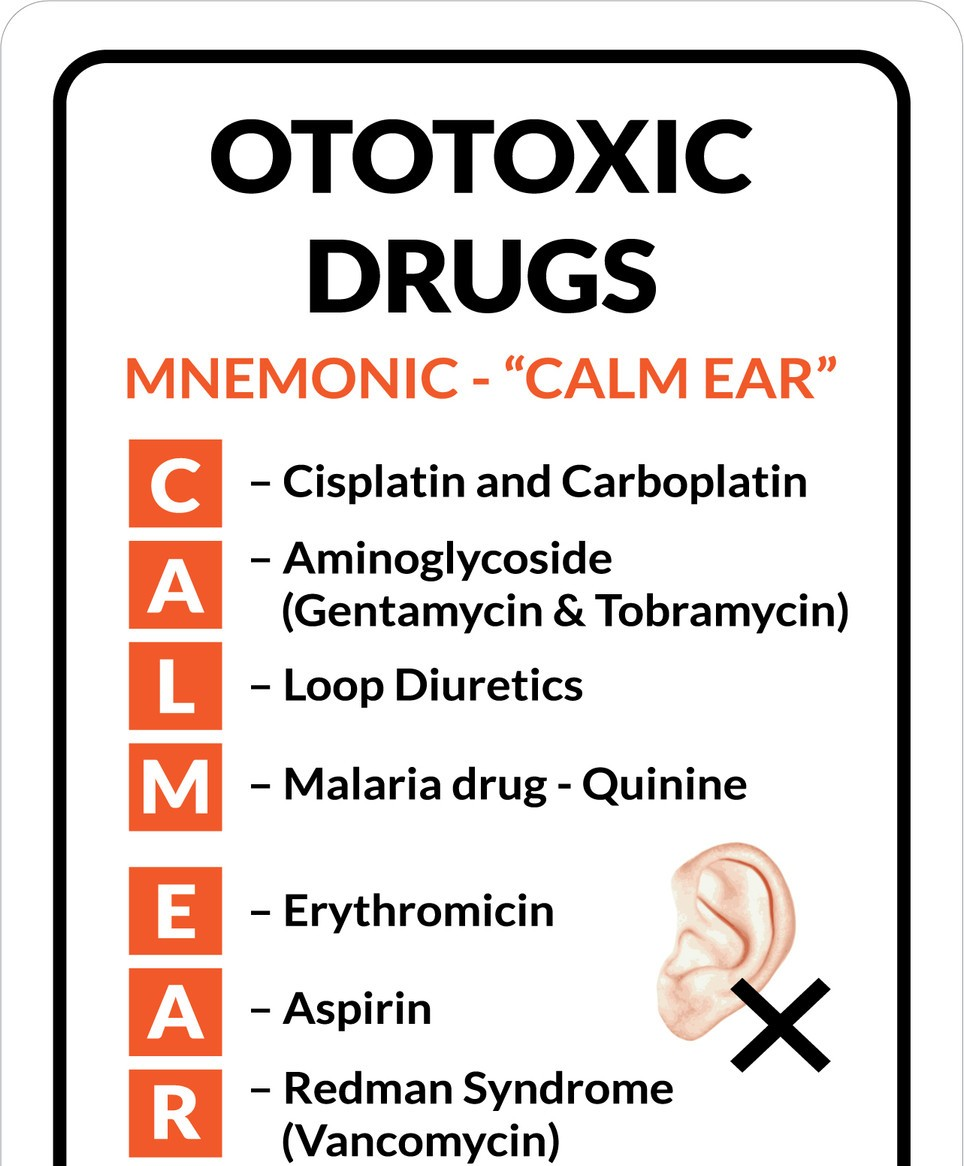
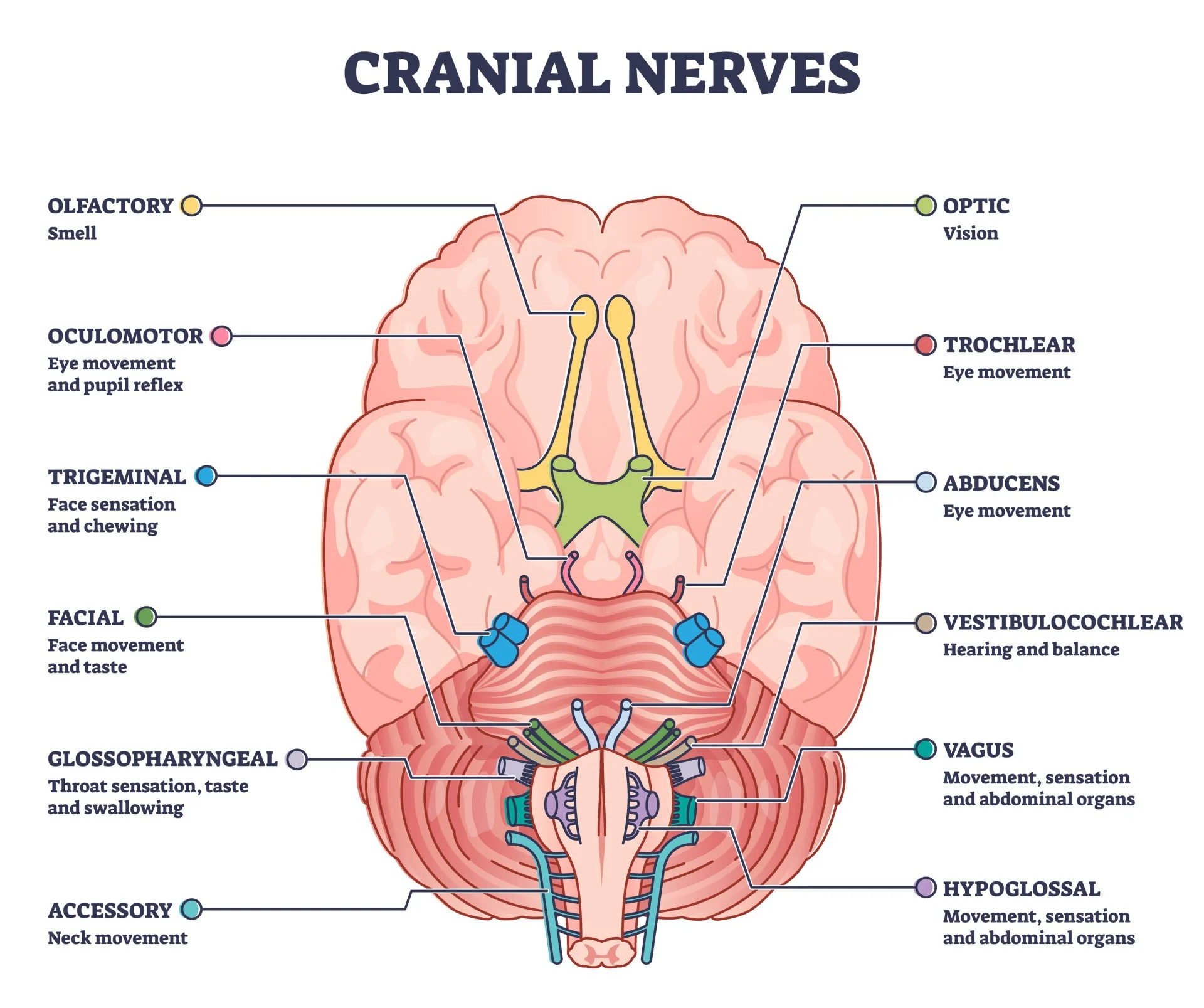
The vestibular disorder, labyrinthitis, results from inflammation or infection from acute febrile (fever) diseases, such as pneumonia, influenza, and especially chronic otitis media or infection of the middle ear. (See Diagnostic Code: 6200 Otitis media). Other causes may be related to ototoxic drugs. Vertigo may result from lesions or disturbances in the inner ear, VIIIth cranial nerve, vestibular nuclei and associated pathways in the brainstem and cerebellum. Vertigo may also be caused by ototoxic conditions related to salicylates, alcohol, or antibiotics. Other causes include: sunstroke; postural hypotension; or toxemia due to food poisoning; and infectious disease.
{kind=link}
{kind=link}
{kind=link}
Signs & Symptoms
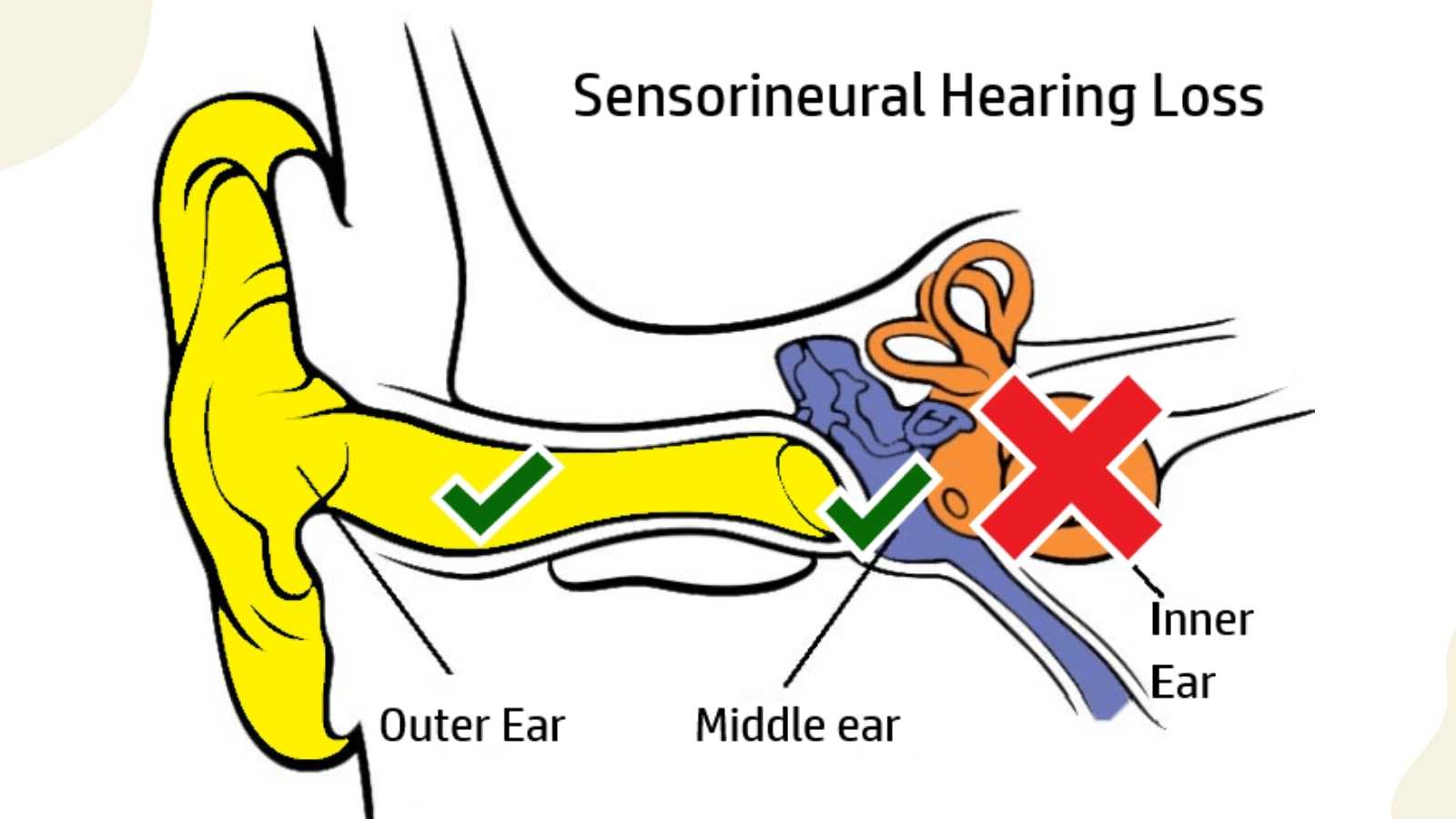
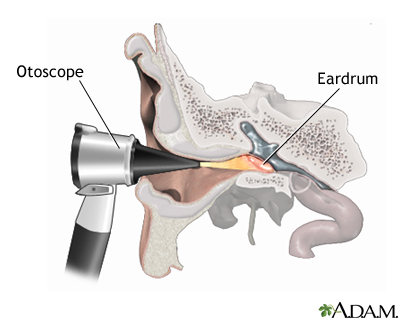
Signs and symptoms of labyrinthitis may include: severe vertigo from any movement of the head; sensorineural hearing loss; spontaneous nystagmus (see Diagnostic Code: 6016 Nystagmus) nausea; vomiting; and giddiness. Otoscopy is usually normal, however there may be purulent middle ear infection. Vertigo may be fleeting or incapacitating, it may last minutes or last as long as 3 to 5 days. The symptoms may include: spinning, disequilibrium, staggering, motion sickness, tinnitus, and hearing loss.
{kind=link}
{kind=link}
Tests
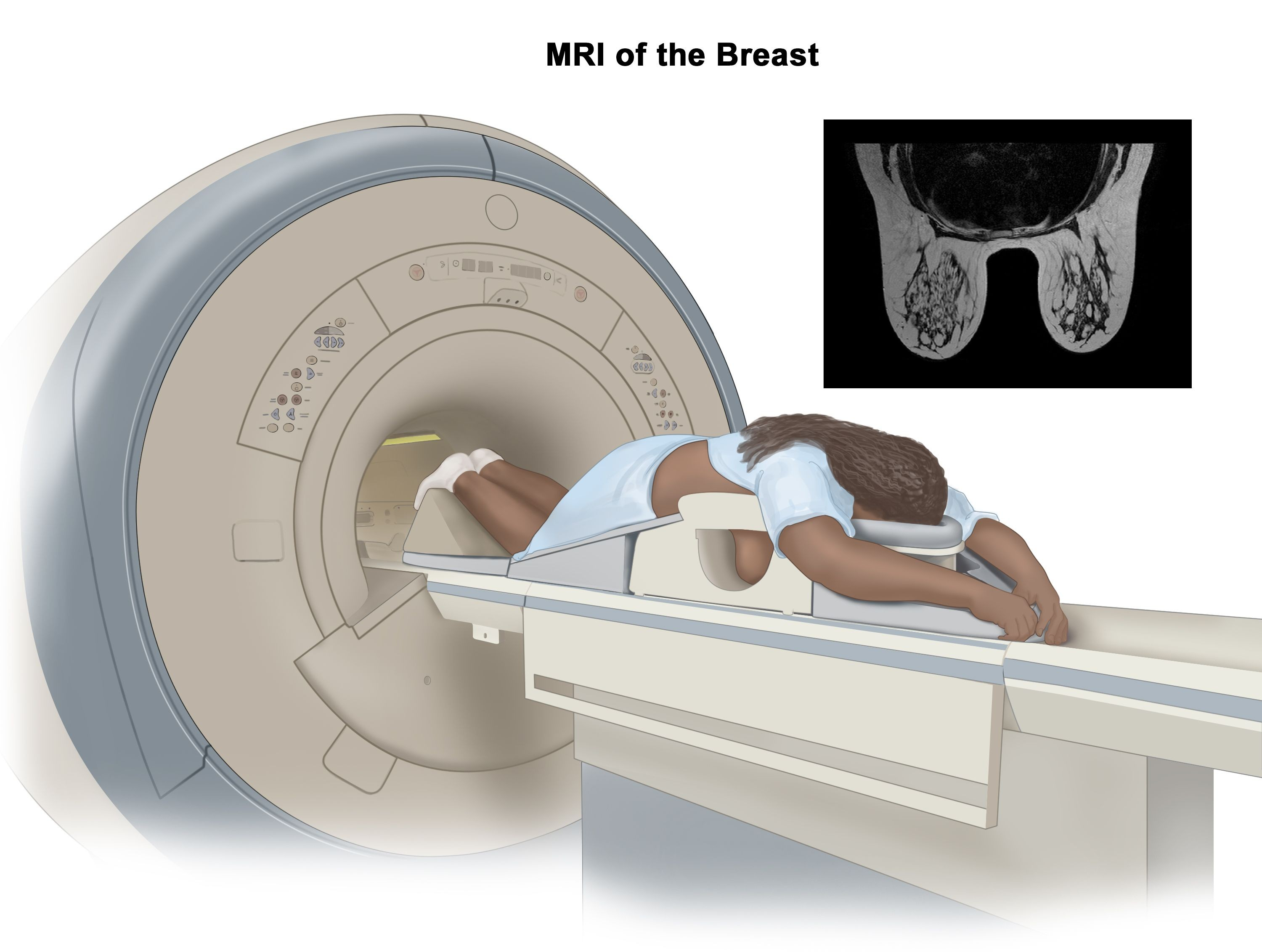
Diagnostic tests include audiometry and culture and sensitivity (C&S) testing (if purulent drainage is present). Other tests may include: x-rays, magnetic resonance imaging (MRI), and electronystagmography (ENG). Tests for vertigo may include, but are not limited to: a neurological examination; Romberg; caloric stimulation test; and tests for nystagmus.
{kind=link}
{kind=link}
Treatment
Treatment includes: bedrest (preferably in the supine position,) antibiotics coupled with oral fluids and possibly intravenous fluids. Medical treatment may include steroids and sedatives that affect the labyrinth. Surgery is rarely indicated.
Residuals
There may be permanent loss of vestibular function requiring rehabilitation exercises and neurosensory hearing loss.
Special Considerations
- Objective findings supporting the diagnosis of vestibular disequilibrium are required before a compensable evaluation can be assigned under this code. Hearing impairment or suppuration shall be separately rated and combined. (38 CFR 4.87 Schedule of ratings-ear)
- Since the symptoms may not be permanent, schedule a future exam if the onset is recent and until stability is reached. Even though the acute symptoms subside quickly in many cases, a person may be left with mild sensitivity to head motion that last for years, and may have recurrent attacks. This is true of both neuronitis and labyrinthitis. Permanent hearing loss occurs, but rarely. (Revision of Rating Schedule: Ear and Other Sense Organs, 1999)
- Compensation is payable for the combinations of service-connected and nonservice-connected disabilities specified in 38 CFR 3.383(a)(3) (see below) as if both disabilities were service-connected, provided the nonservice-connected disability is not the result of the veteran's own willful misconduct.
- Hearing impairment in one ear compensable to a degree of 10 percent or more as a result of service-connected disability and hearing impairment as a result of nonservice-connected disability that meets the provisions of 38 CFR 3.385 in the other ear.
- Objective findings for a compensable evaluation for peripheral vestibular disorder manifested by disequilibrium includes quantitative testing such as electronystagmography (ENG) and auditory brainstem evoked response (ABR) but are not limited to such tests. A variety of clinical examination maneuvers also are used to test for disequilibrium and positive results to examination maneuvers are also considered objective evidence in support of the diagnosis of vestibular disequilibrium.
- If audiometric testing results contain a value above 105 decibels, enter the value into the hearing loss calculator at no higher than 105 decibels for the purpose of determining the puretone threshold average as directed by VA's Handbook of Standard Procedures and Best Practices for Audiology Compensation and Pension Examinations.
- For the purpose of assigning a disability percentage for hearing loss always enter air conduction results into the hearing loss calculator within VBMS-R.
Notes
- Objective findings supporting the diagnosis of vestibular disequilibrium are required before a compensable evaluation can be assigned under this code. Hearing impairment or suppuration shall be separately rated and combined.
- Consider whether the evidentiary record shows that objective examination results or other tests were cited and support the diagnosis of the peripheral vestibular disorder manifested by disequilibrium.